
IV STEM CELLS AND EXOSOMES
We Specialize In Getting Your Life Back
While regenerative medicine shows promise in the rapidly growing body of scientific data, it has yet to be proven to be effective and it is not FDA-approved. All procedures are entirely elective.
We are very careful to only work with patients that we think we have a chance of helping based on our experience. Namely, patients who are in overall good health who suffer from chronic pain caused by damaged or degenerated musculoskeletal tissues (such as joints, spine, or ligaments), that is not “too far gone”. While we have helped many people, there are people we have worked with that we have not helped at all. Our experience is that overall, we help more people than we don’t help, but there is nothing about regenerative medicine that is either a “miracle” or a “cure”.
Florida IV Stem Cells – Frequently Asked Questions
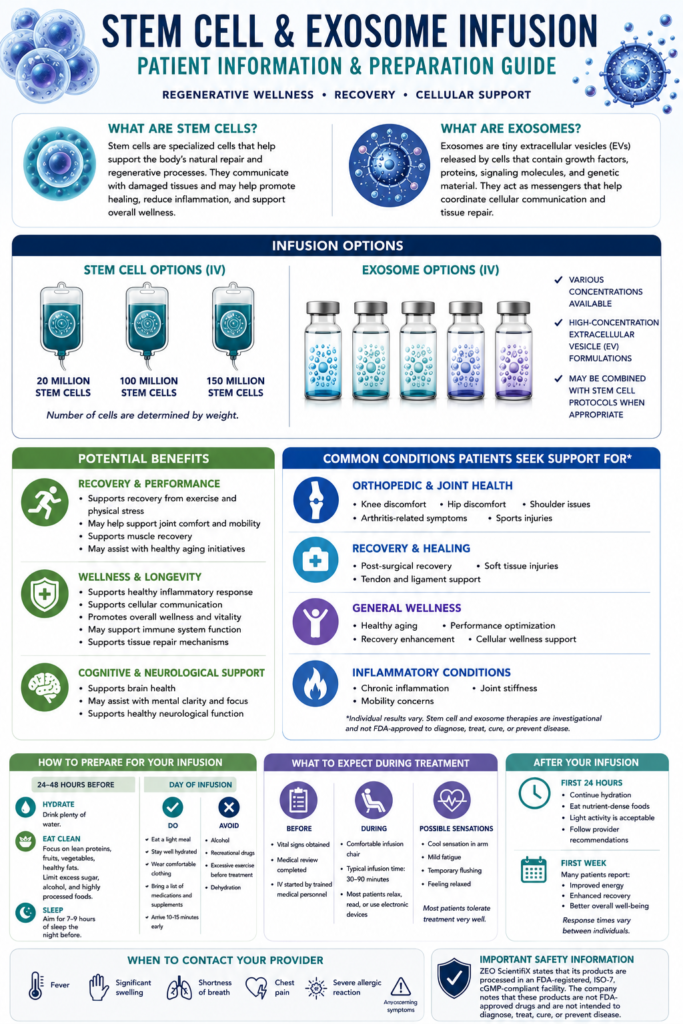
IV Stem Cells (Mesenchymal Stem Cells / MSCs)
What they are: Living, fully intact, replicating cellular entities from umbilical cord
The Mechanism: MSCs are structural “builders.” While they do not permanently engraft or turn into new organs, they physically home to areas of acute injury or chronic inflammation. Once there, they stay alive in the tissues for days or weeks, acting as continuous, smart “bioreactors” that release tailored healing signals in response to the microenvironment.
Primary Benefit: Maximum potency for structural damage, deep joint repair, severe tissue degradation, and complex systemic conditions requiring a sustained, long-term cellular response.
IV Stem Cell Exosomes (Extracellular Vesicles / EVs)
What they are: Non-living, acellular, microscopic lipid “bubbles” (30–150 nanometers) naturally secreted by stem cells.
The Mechanism: Exosomes are pure “messengers.” They do not contain live cells, DNA, or the ability to replicate. Instead, they are packed with a concentrated payload of growth factors, cytokines, mRNA, and microRNA. They float through circulation, fuse with the patient’s existing cells, and instantly deliver “blueprints” instructing those native cells to downregulate inflammation and accelerate self-repair.
Primary Benefit: High safety profile and immediate cellular signaling. Because they are non-living, they carry zero risk of replication or tumor formation, have exceptionally low immunogenicity.
IV Stem Cells (Mesenchymal Stem Cells / MSCs)
What they are: Living, fully intact, replicating cellular entities from umbilical cord
The Mechanism: MSCs are structural “builders.” While they do not permanently engraft or turn into new organs, they physically home to areas of acute injury or chronic inflammation. Once there, they stay alive in the tissues for days or weeks, acting as continuous, smart “bioreactors” that release tailored healing signals in response to the microenvironment.
Primary Benefit: Maximum potency for structural damage, deep joint repair, severe tissue degradation, and complex systemic conditions requiring a sustained, long-term cellular response.
IV Stem Cell Exosomes (Extracellular Vesicles / EVs)
What they are: Non-living, acellular, microscopic lipid “bubbles” (30–150 nanometers) naturally secreted by stem cells.
The Mechanism: Exosomes are pure “messengers.” They do not contain live cells, DNA, or the ability to replicate. Instead, they are packed with a concentrated payload of growth factors, cytokines, mRNA, and microRNA. They float through circulation, fuse with the patient’s existing cells, and instantly deliver “blueprints” instructing those native cells to downregulate inflammation and accelerate self-repair.
Primary Benefit: High safety profile and immediate cellular signaling. Because they are non-living, they carry zero risk of replication or tumor formation, have exceptionally low immunogenicity.
Florida law is incredibly strict about patient safety. Only fully licensed medical doctors (MD) or osteopathic physicians (DO) are legally permitted to perform stem cell therapies. Under Florida law, nurse practitioners (NPs), physician assistants (PAs), or medical assistants cannot independently prescribe or administer these treatments. Every single procedure in our clinic is overseen and executed directly by a licensed physician.
Physicians are strictly restricted to using stem cell therapies for three specific clinical areas:
Orthopedics (e.g., joint degeneration, cartilage wear, ligament tears)
Pain Management (e.g., chronic back pain, systemic joint pain, arthritis)
Wound Care (e.g., non-healing ulcers, severe tissue damage, chronic skin wounds)
We only treat patients for orthopeadic, wound care and pain management but patients commonly report other benefits with IV stem cells such as :
- Chronic inflammation
- Joint and muscle discomfort
- Autoimmune conditions
- Brain fog and cognitive support
- Neurological wellness
- Immune system regulation
- Recovery after illness
- General wellness optimization
Individual results vary and stem cell therapy is not FDA-approved to treat, cure, or prevent disease.
Because live stem cells are robust, dynamic “bioreactors” that home to tissues and secrete healing factors for weeks or even months, they do not require frequent administration.
Wellness & Longevity: Once every 6 to 12 months is standard.
Chronic Inflammatory or Autoimmune Support: An initial loading phase of 2 to 3 infusions spaced 2 to 3 months apart may be recommended, followed by annual maintenance.
Intravenously infused MSCs remain alive and physically present in the patient’s tissues for 2 to 4 weeks.
The Signaling Ripple Effect: The massive blast of instructions delivered by the stem cells during their first month alters the genetic expression of the patient’s own local tissue cells.
The Outcome: The stem cells essentially wake up the patient’s dormant native cells, forcing them to downregulate chronic inflammation and restart self-repair. Because of this cellular “reprogramming,” patients routinely continue to experience clinical improvements, increased energy, and pain reduction for 3 to 6 months (and sometimes up to a year) after a single infusion, long after the original donor cells are completely gone.
The ideal dose depends on:
- Body weight
- Age
- Health goals
- Severity of symptoms
- Treatment protocols
A general rule of thumb is 1 Million to 2 Million MSCs per kilogram of body weight for comprehensive or chronic therapeutic outcomes.
Common IV doses include:
| Goal | Typical Dose |
|---|---|
| General wellness | 25-50 million cells |
| Longevity optimization | 50-100 million cells |
| Autoimmune support | 100-200 million cells |
| Neurological support | 100-300 million cells |
Rejection: The Mesenchymal Stem Cells (MSCs) used in these protocols are ethically sourced from regulated, pristine umbilical cord tissue (maternal donors post-healthy C-section). These cells are immune-privileged, meaning they do not express the surface proteins that trigger an immune rejection. The body does not recognize them as foreign.
Downtime: There is virtually zero downtime. Patients can return to their normal daily activities immediately following the gravity drip. Some patients report a mild, temporary “flu-like” feeling or fatigue for 24 hours post-infusion, which is a completely normal sign that the immune system is actively responding to the new regenerative signaling.
Co-infusing live stem cells and exosomes during the same session provides a powerful “dual-phase signaling” effect. It offers the patient the absolute highest tier of regenerative therapy by delivering a rapid action phase paired with a long-term engine
Advantages include:
- Enhanced cellular communication
- Greater anti-inflammatory support
- Improved tissue signaling
- Increased regenerative potential
- Stronger recovery response
- Improved stem cell activation and survival
Think of stem cells as the “workers” and exosomes as the “instructions” that help direct the repair process.
Stop All NSAIDs (14 Days Prior): Patients must completely discontinue ibuprofen (Advil, Motrin), naproxen (Aleve), celecoxib (Celebrex), and high-dose aspirin.
Safe Alternative: If the patient experiences pain during this window, oral Acetaminophen (Tylenol) is acceptable, as it acts centrally and does not suppress peripheral inflammatory homing signals
Stop Corticosteroids (4–6 Weeks Prior): Oral steroids (like Prednisone) or recent localized joint steroid injections profoundly suppress stem cell activity and must be cleared well in advance.
Hydration Loading: Instruct the patient to drink at least 64 to 80 ounces of water daily for the entire week leading up to the appointment. Excellent hydration expands blood volume, facilitates smooth IV delivery, and supports cell membrane integrity.
Vitamin D3 Maximization: Ensure the patient is supplementing with Vitamin D3. The clinical goal is a serum level between 40-60 ng/ml, which heavily supports stem cell self-renewal and healthy lineage differentiation.
The Toxicity Ban (72 Hours Prior): Strict avoidance of alcohol and nicotine
Administer Oral Pre-Medications: 30 to 60 Minutes Before Drip.
Give Acetaminophen 500 mg–1,000 mg PO to blunt potential transient febrile reactions (chills/fever) and Diphenhydramine 25 mg PO or slow IV push to mitigate early hypersensitivity to the cell-suspension media.